What is a Patellofemoral Injury?
The knee is the largest and one of the most complex joints in the human body. It consists of 4 bones, multiple ligaments, muscles and tendons, cartilage and soft tissue. The knee is a modified hinge joint allowing primary motions of knee flexion and extension. The joint and its components function together to provide stability and power for activities of daily living and athletic movements. However, any of these structures can be injured or damaged requiring treatment as easy as bracing, rest and therapy to as complex as surgery to correct. Regardless, either treatment will typically allow a full return to activity or sports without additional complications.
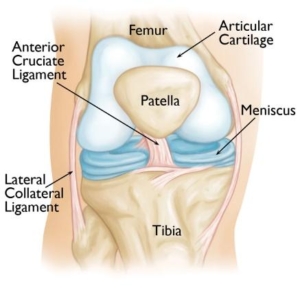
The boney structures of the knee consist of the patella (knee cap), Femur (thigh bone), Tibia and Fibula (lower leg bones). The patella glides with knee flexion and extension within the trochlear groove. Gliding of this area is accomplished through articular cartilage, one of the two types of cartilage within the knee complex. Articular cartilage is the protective covering over the ends of the bones. This allows the joint to glide permitting fluid motion during active and passive activities.
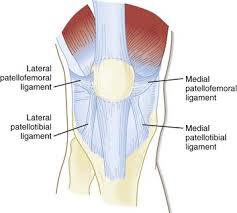
The gliding motion of the patella is stabilized with the additional soft tissue structures such as ligaments, muscles, tendons, synovial tissue and the fat pad beneath the patella. Patellofemoral ligaments are connective bands that stabilize the joint from unwanted movements such as subluxations and dislocations. The lateral and medial patellofemoral ligaments, as seen below, are the main two stabilizing ligaments of the patella.
As you can see, patellofemoral symptoms are located within the front or anterior aspect of the knee. Terms such as chondromalacia patella, jumper’s knee, and runner’s knee are common terminology. However additional problems can also exist such as patellofemoral tilt syndrome and patellofemoral instability. Many conditions related to patellofemoral pain are a result of overuse. Squatting, lunging, running and jumping cause repetitive stress to this area creating unwanted inflammation and pain. In addition to the repetitive stresses, muscular imbalances, muscular tightness or weakness can be a contributing factor to these symptoms.
Signs and Symptoms
Signs and Symptoms of patellofemoral pain are most commonly associated with a dull ache overlying the patella (knee cap). Typically begins gradually and as activity continues symptoms worsen. As they worsen the dull ache can become sharp. They can become debilitating especially with repetitive climbing, squatting, jumping and lunging. Bouts of instability may occur from pain and weakness. Instability, cracking, popping, grinding, stiffness with prolonged sitting and swelling can exist with these conditions.
Diagnosis
Diagnosis will be determined through a thorough history and physical examination by a trained sports medicine and orthopedic knee specialist. Examination will consist of palpating the knee complex for pain and a visual examination for deformities. The clinician will check both active and passive range of motion. Specific manual tests will be performed by the specialist to determine if inflammation exists, the amount of weakness, instability and other possible factors causing symptoms. Once the initial diagnosis has been made, radiological examinations may need to take place for further assessment. X-rays of the knee complex may be ordered to evaluate patellar alignment and also to determine if any other bony conditions exist such as fracture or loose body. If additional concerns from initial exam and assessment are present an MRI (3 dimensional picture) may be ordered to assist in determining the final diagnosis and prognosis.
Treatment
Treatment for all patellofemoral conditions is typically treated non-operatively. Non-surgical management includes rest, ice, compression, anti-inflammatory or narcotics medications, decrease or change of activity level, weight loss, physical therapy, therapeutic taping and bracing. Surgical management through arthroscopy occurs when a small camera is placed into the knee joint to visualize the damage. During this visualization, ligaments, articular cartilage, meniscus and other soft tissue structures are evaluated. Once the assessment has been completed the surgeon uses a variety of instrumentation to repair, or debride (clean) the knee complex.
Rehabilitation
Rehabilitation is recommended for both surgical and non-surgical management. Regardless of your treatment choice, your sports medicine physician will determine a personalized treatment program that fits your needs. Following the initial onset of signs and symptoms, the initial goal is to reduce pain, increase mobility and range of motion. At home and physical therapy, the use of ice, modalities and specific range of motion and strengthening exercises will be performed several times throughout the day. Pain and anti-inflammatory medication may also be prescribed for additional benefit. Crutches and bracing may be initialized following your assessment to aid in stability and prevent further damage to the knee complex. Typically, many will see improvement in symptoms within the first 2-6 weeks following the beginning of conservative treatments.