What is a Rotator Cuff Tear?
Large Rotator Cuff Repair
Surgery performed by Dr. Chams
Knotless Rotator Cuff Repair
3D Surgical Animation
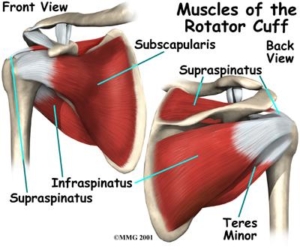
The shoulder complex is a ball and socket joint and is comprised of muscles, bones and several soft tissue structures. The main movers of the shoulder joint are the 4 muscles of the rotator cuff. The rotator cuff consists of the supraspinatus, infraspinatus, teres minor and subscapularis. The rotator cuff works together to provide additional stability and movement of the shoulder complex including shoulder elevation, internal and external rotation.

Rotator cuff tears often occur more frequently in the adult population over the age of 50. Injuries to this structure can occur from an acute traumatic event, such as fall, or they can occur over time called degeneration. Degenerative tears occur from anatomical variants such as bone spurs, decreased blood supply to the rotator cuff as we age although, some rotator cuff exercises have been shown to decrease the chance of injury over time. Historically, many injuries related to the rotator cuff occur from both external factors (trauma) and internal factors (anatomical).
Symptoms
Symptoms can vary but most will have pain and rest and particularly at night. Decreased range of motion due to weakness vs stiffness. Popping, grinding and pain lifting. Visual atrophy or thinning of the muscles about the shoulder may appear. Some can even feel a tear or pop in the shoulder when injury occurs.
Diagnosis
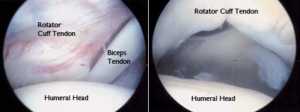
Diagnosis will be determined through a thorough history and physical examination by a trained sports medicine and orthopedic shoulder specialist. Examination will consist of palpating the shoulder complex for pain and a visual examination for deformities. The clinician will check both active and passive range of motion. Specific manual tests will be performed by the specialist to determine if inflammation exists, the amount of weakness and other possible factors causing symptoms. Once the initial diagnosis has been made, an MRI (3 dimensional picture) will be ordered to confirm the diagnosis and assist in determining the severity of the injury. Occasionally, X-rays of the shoulder complex will be ordered to determine if any bony conditions exist prior to your MRI. The MRI photo below demonstrates a full thickness rotator cuff tear.

Severity of rotator cuff tears come in several grades and distinctions and treatments for each vary. Grades are determined by the thickness of the rotator cuff tear. Low grade tears are tears that have less than 25% of the rotator cuff in which it is torn. Moderate grade tears are 25-50% of which the rotator cuff is torn and high grade tears are 50% to 99% in which the rotator cuff is torn. These are also called partial thickness tears. Full thickness tears involve 100% of the tendon of the rotator cuff. MRI’s performed will give your specialist additional information for an accurate diagnosis.
Treatment
Treatment goals are to increase strength, decrease pain and improve functionality of the shoulder complex. These results can be obtained through either conservative or with surgical management. A specific individualized treatment program will be created from your thorough history, physical examination and radiological testing. Conservative management of partial thickness tears can consist of a modification of activity and possibly rest, anti-inflammatory medications, a cortisone injection, orthobiologics such as PRP or Stem Cell injections and formal physical therapy. Surgical management for both partial and full thickness tears may be recommended depending on the severity and size of the rotator cuff tear. Rotator cuff tears are surgically repaired though arthroscopy.
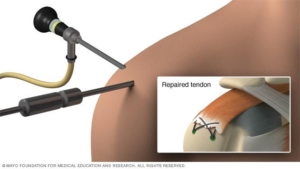
Shoulder Arthroscopy
Shoulder arthroscopy, occurs when a small camera is placed into the shoulder joint to visualize the damage. During this visualization, ligaments, bones and muscles of the shoulder complex are further assessed by the orthopedic surgeon. Once the assessment has been completed the surgeon uses a variety of instrumentation to repair the rotator cuff within the shoulder. The rotator cuff is reattached with either a bio-composite or titanium anchor. From this anchor come three non-dissolvable sutures that are intertwined into the rotator cuff. This allows the surgeon to reattach the rotator cuff to its original location for healing. Augmentation of the rotator cuff repair can also be performed at the end of the procedure with orthobiologics such as PRP (platelet rich plasma) injections or Stem cell injections.

Rehabilitation
Rehabilitation post operatively will begin immediately. Patients will be placed into a sling for 4-8 weeks pending the size of the initial tear and post-surgical repair. A home exercise program will begin immediately following surgery. These exercises will be performed until formal rehabilitation can begin two weeks following surgery. A physical therapist will begin your formal rehabilitation through a planned rehabilitation protocol The size of the rotator cuff tear and quality of the tissue will determine the exact protocol to be followed. By following one of the three protocols determined during your procedure, a small, moderate/large or global rotator cuff repair protocols will be followed by the physical therapist. Initially the physical therapist will advance pain-free passive range of motion. This pain-free range of motion will be obtained within the first 8-12 weeks. During the healing phase of the rotator cuff, which takes 4 months, no active motion of the shoulder will be allowed, as active motion is detrimental to the repair. During this time, progressive strengthening will occur including parascapular and isometric strengthening of the rotator cuff. Active motion and strengthening of the shoulder complex will begin around the 16 week post-operative phase per therapeutic protocol. Total recovery from rotator cuff repairs can typically range from 6-8 months.